Heel Pain The Causes, Indications And Cure Options
Overview

Heel Pain is usually focused on the underside or the back of your heel. If your pain is on the underside of your heel, its likely cause is plantar fasciitis. Pain on the back of your heel, where the Achilles tendon attaches to the heel bone, is Achilles tendinitis. Although heel pain is rarely a symptom of a serious condition, it can interfere with your normal activities, particularly exercise.
Causes
Common causes of heel pain include Achilles tendinitis, Achilles tendon rupture, Bone tumor, Bursitis, Fibromyalgia, Fracture, Gout, Heel pad wear and tear, Heel spur, Osteomyelitis, Peripheral neuropathy, Pinched nerve, Plantar fasciitis, Rheumatoid arthritis, Stress fractures, Tarsal tunnel syndrome, Tendinitis. Causes shown here are commonly associated with this symptom. Work with your doctor or other health care professional for an accurate diagnosis.
Symptoms
Plantar fascia usually causes pain and stiffness on the bottom of your heel although some people have heel spurs and suffer no symptoms at all. Occasionally, heel pain is also associated with other medical disorders such as arthritis (inflammation of the joint), bursitis (inflammation of the tissues around the joint). Those who have symptoms may experience ?First step? pain (stone bruise sensation) after getting out of bed or sitting for a period of time. Pain after driving. Pain on the bottom of your heel. Deep aching pain. Pain can be worse when barefoot.
Diagnosis
Your GP or podiatrist (a healthcare professional who specialises in foot care) may be able to diagnose the cause of your heel pain by asking about your symptoms and examining your heel and foot. You will usually only need further tests if you have additional symptoms that suggest the cause of your heel pain is not inflammation, such as numbness or a tingling sensation in your foot - this could be a sign of nerve damage in your feet and legs (peripheral neuropathy), your foot feels hot and you have a high temperature (fever) of 38C (100.4F) or above - these could be signs of a bone infection, you have stiffness and swelling in your heel - this could be a sign of arthritis. Possible further tests may include, blood tests, X-rays - where small doses of radiation are used to detect problems with your bones and tissues, a magnetic resonance imaging (MRI) scan or ultrasound scan, which are more detailed scans.
Non Surgical Treatment
Depending on the underlying cause, treatment can include. Rest from activities that stress the heel (such as running and jumping). Ice packs. Regular foot massage, concentrating on the arch of the foot. Professional strapping. A splint worn at night. Flexibility exercises. Ultrasound therapy. Anti-inflammatory medicine (topical or oral). Checking your posture and walking style, to correct imbalances and gait abnormalities that may contribute to the pain. Shoe inserts (orthoses) to help support the foot. In some cases, surgery may be recommended to treat conditions including neuroma, bursitis and heel spurs.
Surgical Treatment
Surgery is a last resort in the treatment of heel pain. Physicians have developed many procedures in the last 100 years to try to cure heel pain. Most procedures that are commonly used today focus on several areas, remove the bone spur (if one is present), release the plantar fascia (plantar fasciotomy), release pressure on the small nerves in the area. Usually the procedure is done through a small incision on the inside edge of the foot, although some surgeons now perform this type of surgery using an endoscope. An endoscope is a tiny TV camera that can be inserted into a joint or under the skin to allow the surgeon to see the structures involved in the surgery. By using the endoscope, a surgeon can complete the surgery with a smaller incision and presumably less damage to normal tissues. It is unclear whether an endoscopic procedure for this condition is better than the traditional small incision. Surgery usually involves identifying the area where the plantar fascia attaches to the heel and releasing the fascia partially from the bone. If a small spur is present this is removed. The small nerves that travel under the plantar fascia are identified and released from anything that seems to be causing pressure on the nerves. This surgery can usually be done on an outpatient basis. This means you can leave the hospital the same day.
Prevention

Wear shoes that fit well, front, back and sides and have shock-absorbent soles, rigid uppers and supportive heel counters. Do not wear shoes with excessive wear on heels or soles. Prepare properly before exercising. Warm-up before running or walking, and do some stretching exercises afterward. Pace yourself when you participate in athletic activities. If overweight, try non weight-bearing activities such as swimming or cycling. Your podiatrist may also use taping or strapping to provide extra support for your foot. Orthoses (shoe inserts) specifically made to suit your needs may be also be prescribed.
Coping With Achilles Tendinitis
Overview
 The Achilles tendon, which connects the calf muscles to the heel bone, can withstand significant pressure from physical activities. Achilles tendinitis is estimated to account for approximately 11 percent of all running injuries, as the Achilles tendon provides the momentum to push off to walk or run. Achilles tendinitis, also called Achilles tendinopathy, results from overuse, injury or disease of the Achilles tendon, which causes the area to become inflamed. There are two types of Achilles tendinitis: Non-insertional Achilles Tendinitis - Fibers that are located in the middle portion of the tendon began to develop small tears that cause swelling and thickening. This type of tendinitis is usually found in younger people who are very active. Insertional Achilles Tendinitis - Develops where the tendon attaches to the heel bone in the lower part of the heel. Extra bone growth also called bone spurs form because of this tendinitis and can affect patients at any time, even if they are not active.
The Achilles tendon, which connects the calf muscles to the heel bone, can withstand significant pressure from physical activities. Achilles tendinitis is estimated to account for approximately 11 percent of all running injuries, as the Achilles tendon provides the momentum to push off to walk or run. Achilles tendinitis, also called Achilles tendinopathy, results from overuse, injury or disease of the Achilles tendon, which causes the area to become inflamed. There are two types of Achilles tendinitis: Non-insertional Achilles Tendinitis - Fibers that are located in the middle portion of the tendon began to develop small tears that cause swelling and thickening. This type of tendinitis is usually found in younger people who are very active. Insertional Achilles Tendinitis - Develops where the tendon attaches to the heel bone in the lower part of the heel. Extra bone growth also called bone spurs form because of this tendinitis and can affect patients at any time, even if they are not active.
Causes
As ?overuse? disorders, Achilles tendonitis and tendonosis are usually caused by a sudden increase of a repetitive activity involving the Achilles tendon. Such activity puts too much stress on the tendon too quickly, leading to micro-injury of the tendon fibers. Due to this ongoing stress on the tendon, the body is unable to repair the injured tissue. The structure of the tendon is then altered, resulting in continued pain. Achilles4Athletes are at high risk for developing disorders of the Achilles tendon. Achilles tendonitis and tendonosis are also common in individuals whose work puts stress on their ankles and feet, such as laborers, as well as in ?weekend warriors?-those who are less conditioned and participate in athletics only on weekends or infrequently. In addition, people with excessive pronation (flattening of the arch) have a tendency to develop Achilles tendonitis and tendonosis due to the greater demands placed on the tendon when walking. If these individuals wear shoes without adequate stability, their over-pronation could further aggravate the Achilles tendon.
Symptoms
Achilles tendonitis may be felt as a burning pain at the beginning of activity, which gets less during activity and then worsens following activity. The tendon may feel stiff first thing in the morning or at the beginning of exercise. Achilles tendonitis usually causes pain, stiffness, and loss of strength in the affected area. The pain may get worse when you use your Achilles tendon. You may have more pain and stiffness during the night or when you get up in the morning. The area may be tender, red, warm, or swollen if there is inflammation. You may notice a crunchy sound or feeling when you use the tendon.
Diagnosis
Your physiotherapist or sports doctor can usually confirm the diagnosis of Achilles tendonitis in the clinic. They will base their diagnosis on your history, symptom behaviour and clinical tests. Achilles tendons will often have a painful and prominent lump within the tendon. Further investigations include US scan or MRI. X-rays are of little use in the diagnosis.
Nonsurgical Treatment
Ask your Pharmacist for advice. 1) Your Pharmacy stocks a range of cold packs which may be applied to the area to decrease inflammation. 2) Ask your Pharmacist about a temporary heel raise or pad which can be inserted into footwear to decrease the force absorbed by the tendon when the feet land heavily on the ground. 3) Gently massaging a heat-producing liniment into the calf can help to relieve tension in the muscle which may relieve the symptoms of Achilles Tendinitis. Ask your Pharmacist to recommend the most appropriate type. 4) Gels, sprays or creams which help to reduce inflammation are available and may be applied to the injured area. Ask your Pharmacist for advice. 5) Your Pharmacist can advise you on analgesic, anti-inflammatory medications such as Aspirin which may be of assistance. Aspirin should be avoided in children under the age of 12 and those aged 12 to 15 who have a fever. 6) Strapping the ankle can help restrict movement and minimise further injury. Your Pharmacist stocks a range of athletic strapping tape and ankle guards which may assist your injury.
Surgical Treatment
Open Achilles Tendon Surgery is the traditional Achilles tendon surgery and remains the 'gold standard' of surgery treatments. During this procedure one long incision (10 to 17 cm in length) is made slightly on an angle on the back on your lower leg/heel. An angled incision like this one allows for the patient's comfort during future recovery during physical therapy and when transitioning back into normal footwear. Open surgery is performed to provide the surgeon with better visibility of the Achilles tendon. This visibility allows the surgeon to remove scar tissue on the tendon, damaged/frayed tissue and any calcium deposits or bone spurs that have formed in the ankle joint. Once this is done, the surgeon will have a full unobstructed view of the tendon tear and can precisely re-align/suture the edges of the tear back together. An open incision this large also provides enough room for the surgeon to prepare a tendon transfer if it's required. When repairing the tendon, non-absorbale sutures may be placed above and below the tear to make sure that the repair is as strong as possible. A small screw/anchor is used to reattach the tendon back to the heel bone if the Achilles tendon has been ruptured completely. An open procedure with precise suturing improves overall strength of your Achilles tendon during the recovery process, making it less likely to re-rupture in the future.
Prevention
To lower your risk of Achilles tendonitis, stretch your calf muscles. Stretching at the beginning of each day will improve your agility and make you less prone to injury. You should also try to stretch both before and after workouts. To stretch your Achilles, stand with a straight leg, and lean forward as you keep your heel on the ground. If this is painful, be sure to check with a doctor. It is always a good idea to talk to your doctor before starting a new exercise routine. Whenever you begin a new fitness regimen, it is a good idea to set incremental goals. Gradually intensifying your physical activity is less likely to cause injury. Limiting sudden movements that jolt the heels and calves also helps to reduce the risk of Achilles tendonitis. Try combining both high- and low-impact exercises in your workouts to reduce stress on the tendon. For example, playing basketball can be combined with swimming. It doesn?t matter if you?re walking, running, or just hanging out. To decrease pressure on your calves and Achilles tendon, it?s important to always wear the right shoes. That means choosing shoes with proper cushioning and arch support. If you?ve worn a pair of shoes for a long time, consider replacing them or using arch supports. Some women feel pain in the Achilles tendon when switching from high heels to flats. Daily wearing of high heels can both tighten and shorten the Achilles tendon. Wearing flats causes additional bending in the foot. This can be painful for the high-heel wearer who is not accustomed to the resulting flexion. One effective strategy is to reduce the heel size of shoes gradually. This allows the tendon to slowly stretch and increase its range of motion.
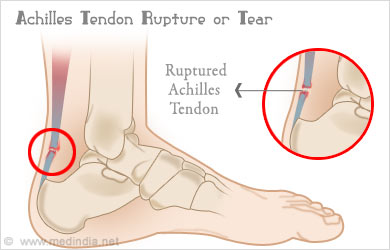
What Are The Signs Of A Ruptured Achilles Tendon?
Overview

Achilles tendon rupture is an injury that affects the back of your lower leg. It most commonly occurs in people playing recreational sports. The Achilles tendon is a strong fibrous cord that connects the muscles in the back of your calf to your heel bone. If you overstretch your Achilles tendon, it can tear (rupture) completely or just partially. If your Achilles tendon ruptures, you might feel a pop or snap, followed by an immediate sharp pain in the back of your ankle and lower leg that is likely to affect your ability to walk properly. Surgery is often the best option to repair an Achilles tendon rupture. For many people, however, nonsurgical treatment works just as well.
Causes
The exact cause of Achilles tendon ruptures is hard to say. It can happen suddenly, without warning, or following an Achilles tendonitis . It seems that weak calf muscles may contribute to problems. If the muscles are weak and become fatigued, they may tighten and shorten. Overuse can also be a problem by leading to muscle fatigue . The more fatigued the calf muscles are, the shorter and tighter they will become. This tightness can increase the stress on the Achilles tendon and result in a rupture. Additionally, an imbalance of strength of the anterior lower leg muscles and the posterior lower leg muscles may also put an athlete at risk for an injury to the Achilles tendon. An Achilles tendon rupture is more likely when the force on the tendon is greater than the strength of the tendon. If the foot is dorsiflexed while the lower leg moves forward and the calf muscles contract, a rupture may occur. Most ruptures happen during a forceful stretch of the tendon while the calf muscles contract. Other factors that may increase the risk of Achilles tendon rupture include. Tight calf muscles and/or Achilles tendon. Change in running surface eg: from grass to concrete. Incorrect or poor footwear. A change of footwear eg: from heeled to flat shoes. It is thought that some medical conditions, such as gout, tuberculosis and systemic lupus erythematosus, may increase the risk of Achilles tendon rupture.
Symptoms
You may notice the symptoms come on suddenly during a sporting activity or injury. You might hear a snap or feel a sudden sharp pain when the tendon is torn. The sharp pain usually settles quickly, although there may be some aching at the back of the lower leg. After the injury, the usual symptoms are a flat-footed type of walk. You can walk and bear weight, but cannot push off the ground properly on the side where the tendon is ruptured. Inability to stand on tiptoe. If the tendon is completely torn, you may feel a gap just above the back of the heel. However, if there is bruising then the swelling may disguise the gap. If you suspect an Achilles tendon rupture, it is best to see a doctor urgently, because the tendon heals better if treated sooner rather than later. A person with a ruptured Achilles tendon may experience one or more of the following. Sudden pain (which feels like a kick or a stab) in the back of the ankle or calf, often subsiding into a dull ache. A popping or snapping sensation. Swelling on the back of the leg between the heel and the calf. Difficulty walking (especially upstairs or uphill) and difficulty rising up on the toes.
Diagnosis
The actual area of an Achilles tendon rupture cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in individuals with an Achilles tendon rupture these x-rays are usually normal. Diagnostic ultrasound of the tendon can be performed to assess the integrity of the tendon. Other diagnostic tests, such as MRI's, may also be required in difficult cases.
Non Surgical Treatment
Once the Achilles tendon is partially damaged, one should exercise great care. The risk of rupture is high and if pain is associated with walking, one should consult with an orthopedic surgeon or a sports physician. A complete rupture of the Achilles tendon is never treated at home. It is important to understand that there are no minerals, nutrients, or herbs to treat Achilles tendon injury and any delay just worsens the recovery.

Surgical Treatment
Surgery will involve stitching the two ends of the tendon together, before placing the leg in a cast or brace. The advantage of having an operation is the reduced chance of the rupture reoccurring, however it will involve the risks associated with any surgical procedure, such as infection.
The Facts Not Misguided Beliefs Concerning Achilles Tendon Rupture
Overview

A torn or ruptured Achilles tendon is simply no fun at all. This essential cord of strong, fibrous material attaches the heel bone to the calf muscles and is used in just about every movement, from walking and running to jumping and standing on your tip-toes. It also helps bend the foot downwards at the ankle. As the strongest tendon in the body, the Achilles can withstand a force of about 1,000 pounds. About 7 out of every 100,000 people will suffer from a ruptured Achilles at some point in time, with over 80% of these injuries occurring during a recreational sports activity. Athletes have a 24% chance of tearing their Achilles, but competitive runners have a 40 to 50% chance of Achilles tendon rupture during their lifetime.
Causes
Your Achilles tendon helps you point your foot downward, rise on your toes and push off your foot as you walk. You rely on it virtually every time you move your foot. Rupture usually occurs in the section of the tendon located within 2 1/2 inches (about 6 centimeters) of the point where it attaches to the heel bone. This section may be predisposed to rupture because it gets less blood flow, which also may impair its ability to heal. Ruptures often are caused by a sudden increase in the amount of stress on your Achilles tendon. Common examples include increasing the intensity of sports participation, especially in sports that involve jumping, falling from a height, stepping into a hole.
Symptoms
If your Achilles tendon is ruptured you will experience severe pain in the back of your leg, swelling, stiffness, and difficulty to stand on tiptoe and push the leg when walking. A popping or snapping sound is heard when the injury occurs. You may also feel a gap or depression in the tendon, just above heel bone.
Diagnosis
The actual area of an Achilles tendon rupture cannot be seen on x-ray. Therefore, although x-rays are often done to rule out bony injuries in individuals with an Achilles tendon rupture these x-rays are usually normal. Diagnostic ultrasound of the tendon can be performed to assess the integrity of the tendon. Other diagnostic tests, such as MRI's, may also be required in difficult cases.
Non Surgical Treatment
Two treatment options are casting or surgery. If an Achilles tendon rupture is untreated then it may not heal properly and could lead to loss of strength. Decisions about treatment options should be made on an individual basis. Non-surgical management traditionally is selected for minor ruptures, less active patients, and those with medical conditions that prevent them from undergoing surgery. The goal of casting is to allow the tendon to slowly heal over time. The foot and ankle are positioned to bring the torn ends of the tendon close together. Casting or bracing for up to 12 weeks or more may be necessary. This method can be effective and avoids some risks, such as infection, associated with surgery. However, the likelihood of re-rupture may be higher with a non-surgical approach and recovery can take longer.

Surgical Treatment
Debate remains regarding the best form of treatment for a ruptured Achilles tendon. The 2 options are:immobilisation or operation. A recent meta-analysis of scientific studies showed that compared to immobilisation, an operation reduces the risk of re-rupture and allows a quicker return to work. An operation is not without risk and these must be balanced against the benefit of a lower re-rupture rate. Both treatments involve immobilisation for 8 weeks.
Make a Free Website with Yola.